






There are specialized equipment and diagnostic tools which help in diagnosis corneal conditions at an early stage. In addition thee tools give us detailed info about the healthy of the cornea which is useful while performing various procdures upon the cornea. We are Javed Eye Centre are fortunate to have the first and only Diagnostic Tool in Faisalabad called Galilei Dual Scheimpflug Analyzer.
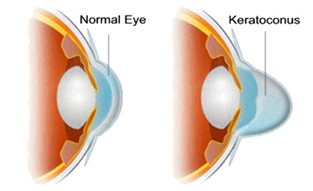
Keratoconus is a rare eye condition in which the normally round, dome-like cornea (the clear front window of the eye) becomes thin and develops a cone-like bulge. Keratoconus literally means “cone-shaped cornea.”

The cornea is a very important part of your eye. As light enters the eye, it refracts, or focuses, the light rays so that you can see clearly. With keratoconus, the shape of the cornea is altered distorting your vision. Keratoconus can make some activities such as driving, typing on a computer, watching television or reading very difficult.
.jpg)
Symptoms of keratoconus?
Keratoconus usually affects both eyes, however; symptoms in each eye may differ. Surprisingly, this is not an eye condition that affects only the elderly. Symptoms usually start to occur in people who are in their late teens and early twenties and may include:
The rate of keratoconus progression varies. It will often progress slowly for 10 to 27 years and then suddenly stop.
What causes keratoconus?
The cause of keratoconus is still not known. Some researchers believe that genetics play a role since an estimated 10% of people with keratoconus also have a family member with the condition.
How is keratoconus treated?
Treatment will often depend on the severity of the condition. During early stages, vision can be corrected with eyeglasses. As the condition progresses, rigid contacts may need to be worn so that light entering the eye is refracted evenly and vision is not distorted. You should also refrain from rubbing your eyes as this can aggravate the thin corneal tissue and make symptoms worse.
When good vision is no longer possible with contact lenses, a corneal transplant is recommended. This surgery is only necessary in about 10-20% of patients with keratoconus. In a corneal transplant, a cornea specialist removes the diseased cornea from your eye and replaces it with a healthy donor cornea. While a corneal transplant will relieve the symptoms of keratoconus, it may not provide you with flawless vision; eyeglasses or contacts may still be needed to achieve your best vision.
The most common type of corneal transplant is known as a penetrating keratoplasty. This involves a full-thickness transplant of the cornea. At times, the diseased or damaged part of the cornea may not involve the entire thickness, and in certain cases, only a partial-thickness transplant is required. This is known as a lamellar keratoplasty. The most common type of lamellar keratoplasty is DSAEK surgery.
![]()
Penetrating keratoplasy involves the surgical removal of the central 2/3rds of the cornea and then the its replacement with an organ donor graft of clear corneal tissue. Unlike other organ transplants, because the cornea does not have blood vessels, donors do not need to be matched to the organ recipient. Developed over 100 years ago, approximately 40,000 corneal transplants are performed each year in the United States.
The Indications
Penetrating or lamellar keratoplasty is indicated when a patient has a scarred or damaged cornea as a result of injury or disease. The damage to a patient’s cornea will result in some amount of vision loss that cannot be corrected with eyeglasses or contact lenses. Some of the more common reasons for a corneal transplant include keratoconus, chemical or traumatic injury to the cornea, genetic corneal dystrophies, or corneal infections caused by viruses, bacteria, or fungi.
The Procedure
Corneal transplants are performed as a day surgery, outpatient procedure. Although you will not be asleep during the procedure, you will be given sedation and a local anesthetic to keep you comfortable throughout the procedure. Dr. Kieval uses a round blade to remove the central 2/3rds of the damaged cornea. An organ donor cornea is then sewn to the remaining cornea with very fine sutures. These sutures are not dissolvable, but rather will stay in place until Dr. Kieval feels it is necessary to remove them. During the surgery patients may feel pressure around the eye, but there is no pain and most patients report that the experience was quite benign. After the procedure a patch will be placed over the eye and you will return home where you are instructed to rest for the remainder of the day.
The Recovery
Your vision will be quite blurry for the first few weeks after surgery as the new cornea is recovering. Afterwards, repeated visits will be necessary to monitor the progress of the transplant and remove sutures in order to optimize your vision. The total visual recovery time for a corneal transplant is often 6 months to a year or longer. Occasionally, a significant amount of astigmatism can occur after a penetrating keratoplasty that eyeglasses alone won’t give adequate vision. These patients may ultimately require contact lenses or additional surgery to reduce or eliminate the astigmatism. Similar to other organ transplants, anti-rejection medications are required for a number of years, however, rather than pills, eye drops are used for this purpose.
Broken sutures, infections, or graft rejection can occur at any time and needs to be addressed immediately.
If at any time the patient experiences redness, pain, loss of vision or any other concerns, our office should be contacted immediately.
About CXL
Before 1998, the only treatment options for keratoconus were custom contact lenses, Intacs and/or corneal transplants. Corneal transplantation is a major surgery performed in an operating room. It involves a doctor making incisions and replacing part of the cornea with corneal graft tissue secured by sutures. As a result, there is a lifelong risk of rejection of the corneal graft as well as the risk of wound rupture, which can lead to permanent loss of vision and, in some cases, loss of the eye
In 1998, doctors in Germany introduced Corneal Collagen Crosslinking with vitamin (riboflavin) eyedrops and UV light (CXL) to treat patients with keratoconus. Today, doctors are performing CXL and successfully treating patients all over the world.
.jpg)
.jpg)
What Does CXL Do?
|
Normal corneas have crosslinks within their collagen fibers that keep it strong and able to retain its normal shape. In keratoconus, the cornea is weak with insufficient structural support |
 |
|
This weakened structure allows the cornea to bulge outwards into irregular shapes which can then cause poor vision, glare and difficulty seeing well enough to drive at night and perform normal activities that require good vision. The crosslinking procedure can add strength to the cornea, making it more stable so it can hold its shape and focusing power. These “links” help strengthen the cornea, which stops the thinning, bulging and further loss of vision. |
|
Who Qualifies for CXL?
To qualify for CXL, patients must be at least 8 years old. To find out if CXL is right for you, visit us for a no-touch, painless screening. During your consultation, the our doctor will determine if CXL might be an option.
What is the CXL Procedure Like?
The CXL treatment is an outpatient procedure performed in the doctor’s office using only numbing eye drops. Before the light is used, the epithelium, a thin layer of clear, protective tissue (like skin) that covers the cornea is prepared for the CXL procedure. Next, vitamin B2 eye drops (riboflavin) are used in the eye and the patient is asked to look at a special blue (ultraviolet) light while lying comfortably on the reclining chair. It’s generally easy for patients to look at this light because the eyes are numb and we use drops to keep the eyes moist. From a patient’s perspective, the UV light appears to have a soft blue color.

Does the CXL Procedure Hurt?
No. The crosslinking procedure is painless. Anesthetic eye drops are used to avoid discomfort during the procedure. Some patients have discomfort after the procedure and your surgeon can tell you whether you are or are not likely to do so and how to ensure your comfort.
How Long Does the Procedure Take?
If two eyes are being treated at once, the procedure takes approximately an hour and a half. If only one eye is being treated at a time, the procedure takes approximately one hour.
Are There Different Technique Options?
In the least invasive CXL treatment called transepithelial (or epi-on) CXL technique, the surface skin layer (epithelium) of the cornea is not removed so the recovery is much faster than the traditional CXL technique. This least invasive technique can only be done on corneas that are thick enough. Your surgeon will be able to determine if you might be a candidate for this less invasive transepithelial (or epi-on) CXL treatment.
Intacs or corneal rings, along with other techniques, can be used to treat astigmatism in keratoconus patients, but they do not stop the progression of the disease. The only treatment that stops progressive vision loss in keratoconus or ectasia is CXL.
Recovery Time from the Procedure
We want to help you get back to your normal life activities as quickly as possible. Based on the treatments that are best you’re your eyes, your doctor can tell you when you can expect to return to your usual activities. With transepithelial (or epi-on) CXL, most people return to their usual activities the next day. With traditional epithelium off CXL, most people can do so after 5-8 days.
When can I resume wearing contact lenses after CXL?
This will depend on how difficult it is for you to see without your contacts, the type of CXL procedure you had, and how fast your eye heals. With transepithelial (or epi-on) CXL, can typically start wearing corrective contact lenses within a few days to a week. With traditional (epi-off, more invasive) CXL, most patients return to wearing contact lenses 2 to 6 weeks after the procedure. Your surgeon will determine how long this might take in your case.
When will I notice improvement in my vision after CXL?
The main purpose of CXL is to prevent further vision loss as it is a mainly preventive treatment. Some patients also get some improvement in their vision as well. Generally, with CXL, visual improvement is a long process. With the less invasive, transepithelial CXL, some patients have found their vision improved somewhat as early as several weeks after treatment. With the traditional (more invasive epi-off) CXL procedure, most patients find that immediately after the cross-linking treatment, their vision is actually worse than it was before the procedure. This usually goes on for roughly 3-6 weeks. Patients may start to notice positive effects 4-8 weeks after the procedure and may experience major improvement in vision at least 3-6 months after the procedure. In some studies, patients’ vision and astigmatism were still continuing to improve five years after the crosslinking procedure.
Long Term Results
Improvement in corneal shape and vision can continue over many years, with some patients noticing further improvement in their quality of vision even 2 to 4 years following the treatment.
How Effective is CXL?
Many research studies have shown that CXL may prevent further vision loss in over 98% of patients and improves vision in over 50% of patients treated.
When is the Best Time to Have CXL?
As with most conditions, prevention of a problem is better than treatment of a problem. The best time to treat keratoconus is before the effects become apparent and vision has been lost. However, this does not mean that people with very poor vision from keratoconus cannot be helped by CXL. The best way to know if you CXL can help you, would be to visit a practicing doctor for a screening.
How Long Does the Effect of CXL Treatment Last?
Based on CXL study results over more than a decade, the beneficial effects of CXL appear to last for many years and there is some evidence that the strengthening effect may be permanent.
Does CXL Need to Be Repeated?
In many studies, the majority of patients responded to a single vitamin and light CXL treatment and did not need to have the procedure repeated. CXL can be repeated if the first treatment is not effective.
Dry Eye Syndrome is the lack of lubrication or moisture in the eyes related to the tear film and production of natural tears. This syndrome can be caused by factors including the natural aging process, cold medicines, contact lens wear, and certain environmental factors.
If you have a dry and scratchy feeling, or a burning sensation, you may be experiencing dry eye. A Schirmer test is conducted to determine the severity of the dryness.
What causes dry eyes?
The exact cause of Dry Eye Syndrome is still being researched by the medical community, but it has been determined that certain elements are known to cause dry eyes. Certain diseases such as lupus, rheumatoid arthritis, or Sjögren’s Syndrome can cause dry eyes. Some prescription medications and over-the-counter medicine can also lead to dry eyes, as well as contact lens wear, and environmental factors. Some medications known to cause dry eyes are antihistamines, such as Benadryl, some blood pressure medications and anti-depressants. Also, if you are a smoker, you are at risk for developing Dry Eye Syndrome.
The Tear Film
The tear film is made up of three different layers: an oily layer, a watery layer and a mucin layer. The small glands on the edge of the eyelid, called meibomian glands, produce the oily layer of the tear film. The oily layer is what smoothes the tear surface and decreases the evaporation of tears. The watery layer is the middle layer and the largest layer. The watery layer is produced by small glands on the conjunctiva which is the membrane lining the inside of the eyelid and covering the eyeball. The innermost layer is the mucus layer produced by goblet cells in the conjuctiva. This layer is what allows the watery layer to spread evenly over the surface of the eye and helps to keep the eye moist.
Treatment Options
Dry Eye Syndrome is difficult to cure, but there are certain treatments to help reduce the effects including:
Home | About Us | Our Doctors | Services | Gallery | Contact Us | News |
© Copyright 2014–2015 All Rights Reserved by Javed Eye Centre.Google+
Developed by Solutions Player (pvt) ltd. ![]()